{kind=link}
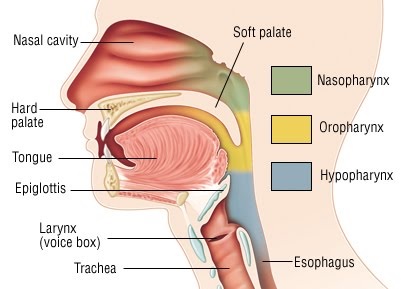
Roohealthcare.com – The Eustachian tube is a narrow hollow tube in the pharynx, originating from the pharynx and descending to merge with the palatopharyngeus muscle. These two muscles work together to elevate the soft palate during swallowing. Both the tensor tympani muscle and tensor veli palatini muscle have motor innervation in the vagus nerve.
The Eustachian Tube Has a Cartilage Skeleton
The Eustachian tube has a cartilaginous skeleton. This section is one piece and is fixed to the basisphenoid bone. There is also a medial cartilaginous lamina, which protrudes into the nasopharynx and provides the skeleton for the posterior cushion known as the torus tubarius. The medial cartilaginous lamina is thick in the nasopharynx and tapers toward the bony cartilaginous junction. The proximal part of the tube is mobile and rotates during tubal dilation.
The tensor tympani and levator veli palatini act laterally and medially to open the Eustachian tube. Bartolomeo Eustachio, an Italian anatomist, is responsible for naming the tube. Although his name is often misspelled, the tube is also known as Eustachio, or Eustachi. The Italian anatomist Bartholomeus Eustachius, also known by the Latin name Bartholomaeus Eustachius, lived in the 1510s-1574.
The Eustachian tube has several factors that affect its optimal function. The length of the tube, its angulation to the horizontal plane, the function of the tensor veli palatini muscle, and the amount of surfactant produced by the pharyngeal zone are some of these factors. Children have more horizontally oriented Eustachian tubes than adults, which makes them more susceptible to upper respiratory infections. When the Eustachian tube is blocked, the fluid behind the eardrum becomes infected.
Eustachian Tube Connects Middle Ear and Pharynx
Electrical and optical stimulation are two main methods used to assess the functioning of the ET muscles. Electrical stimulation involves electrical currents, while optical stimulation uses light. The electrodes are placed near the palate to monitor the opening and closing of the tube. The electrodes are subdermal or made of fiber optic cables. There are no anesthesia issues with this technique. Electrostimulation is the alternative method, which can be a better option for patients with ETD.
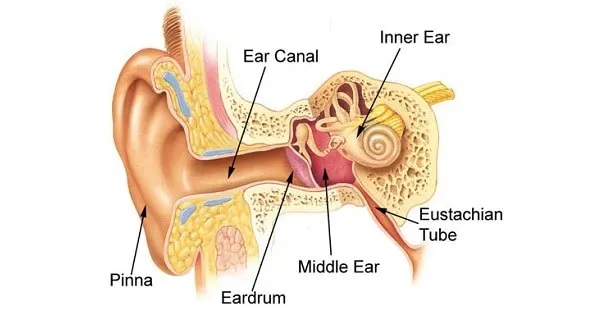
The Eustachian tube connects the middle ear and pharynx. It is essential for normal hearing and functions as a tube. It is also a sophisticated organ, interacting with the surrounding structures and musculature. There are several different types of Eustachian tube muscles, each of which plays a vital role. You may be wondering which one is the most important one.
 Surgery is another option for patients who have a problem with the eustachian tube. This procedure helps to improve the opening and function of the tube. The surgeon inserts cartilage or filler into the opening. After a few months, the patient goes back to a regular doctor for evaluation. The implanted cartilage or filler will increase the opening and function of the eustachian tube.
Surgery is another option for patients who have a problem with the eustachian tube. This procedure helps to improve the opening and function of the tube. The surgeon inserts cartilage or filler into the opening. After a few months, the patient goes back to a regular doctor for evaluation. The implanted cartilage or filler will increase the opening and function of the eustachian tube.
Exercise Worsens Symptoms Due to Increased Breathing Rate
While the Eustachian tube is normally closed, it can open to equalize pressure inside the middle ear. People who can voluntarily contract their Eustachian tube muscles can make their voices louder by wriggling their neck muscles. The tube is essential for airflow because it protects the middle ear. However, if the tube isn’t functioning properly, airflow could be affected.
Patients with PET may experience significant symptoms, including “muffled hearing,” “autophony,” and a constant urge to clear the ear. Other symptoms may include tinnitus, ear fullness, and blockage. Exercise can worsen the symptoms due to increased respiratory rate and decreased blood flow to the eustachian tube muscles. The patient should see a tinnitus specialist for further diagnosis.

There are two types of muscles inside the Eustachian tube. The first, the tensor tympani, arises from the cartilaginous portion of the eustachian tube. The second, the levator palatini, originates from the adjacent portion of the greater sphenoid bone. This muscle inserts onto the handle of the malleus.
Reference: