{kind=link}
Roohealthcare.com – Anterior lumbar fusion is a procedure that replaces one or more spinal discs. During this procedure, a surgeon makes multiple one-inch cuts into the discs to gain access to the spinal cord. Once inside, the bone graft material is packed into a cage and held in place with surgical hardware. The graft will fuse the vertebrae. Once complete, the patient may return to work.
Inhibits New Bone Growth in the Spine
After surgery, the patient will be awakened in a recovery room. They will be given medications and instructed to continue with light activity. This can take up to two to three months to complete. After the surgery, patients should have help for the first 24 to 48 hours. They should avoid strenuous activities or lifting anything more than 5 pounds. Smoking and nicotine use are also not recommended after surgery, because they inhibit the growth of new bone in the spine.
The anterior approach to anterior lumbar fusion is performed through a large incision made in the middle of the lower back. The muscles of the spine are then pushed to one side to make way for the surgeon to see the spine. The lamina of the vertebrae is removed to relieve pressure on the nerve roots. Some of the factors that cause pressure on the nerves include bony spurs, bulging discs, or thickening of ligaments. Once the nerves are free from pressure, the fusion is completed.

As with any surgery, patients should expect some pain after an anterior lumbar fusion. Patients should discuss the intensity and duration of any pain with their surgeon, and ask about pain management options. If pain is unbearable, a rigid body brace may be needed to help alleviate the pain. The patient should also be aware of the possible risks associated with metal hardware after a lumbar fusion. The American College of Cardiology and the American Heart Association has published guidelines on perioperative cardiac evaluation. Surgical risk assessment is based on clinical and physiological factors.
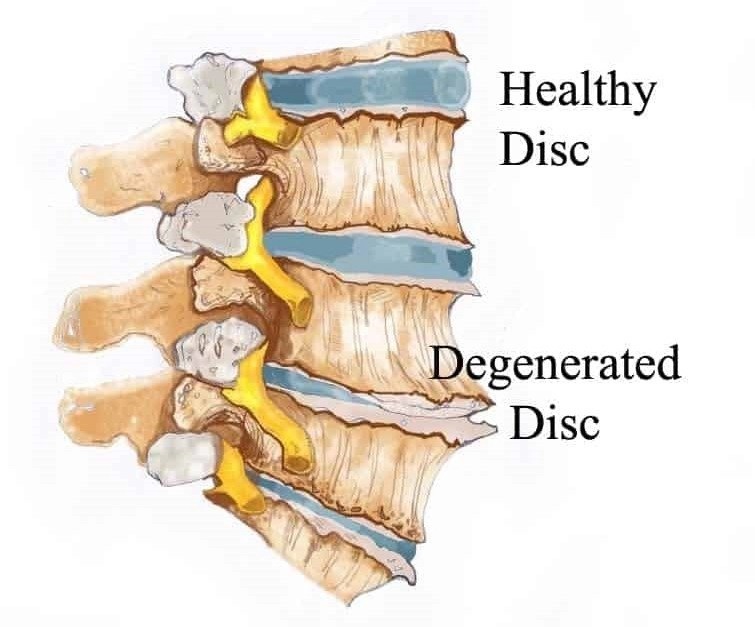
Treating Degenerative Discs in the Lower Back
The primary goal of anterior lumbar fusion is to treat degenerated or unstable discs in the lower back. The surgeon removes intervertebral discs and a bone spacer. Multiple discs may also be removed in an anterior lumbar fusion procedure. The surgery may also include posterior decompression and instrumentation. Anterior lumbar fusion is a common surgical procedure for treating degenerative discs in the low back.
Although the procedure has limited evidence, it is an effective treatment for patients suffering from chronic back pain, radiculopathy, and neurogenic claudication. It is a safer alternative to lumbar fusion performed through the posterior approach. The procedure was first described in 1932 by Capener and has evolved to become a common surgical approach for various lumbar degenerative disorders. These findings indicate that patients can return to their daily activities and enjoy their hobbies.
Potential Risks of Failed Procedures Causing Complications
The procedure typically takes approximately two hours to complete. Patients may be asked to wear a lumbar brace after surgery, while some are given a rigid lumbar corset. Patients are encouraged to keep the wound area clean and dry. Immediately after surgery, patients may take a shower but should cover the surgical area with a bandage. Once the wound has healed, the patient may take a bath. Recovery time from surgery is approximately 2 weeks.
Anterior exposure involves opening the chest to the abdomen. The biggest risk is the possibility of damage to the big arteries. A general surgeon will typically move the abdominal organs out of the way. The procedure can be very complex and complicated, so a general surgeon should perform it with utmost care. Bone morphogenic protein is the synthetic substance that is used in the procedure. It helps to spur the growth of new bone and reduces the chance of a fusion not taking. In addition, it can reduce the need for a bone graft.

However, patients should be aware of the potential risks of the procedure. A failed surgery can lead to complications, such as non-union, as the bone graft may not properly fuse the vertebrae. This could result in postoperative neck pain and decreased patient satisfaction. Further, the bones may shift and cause additional pain after the surgery. Another possible risk is excessive pressure on the graft. This may require another surgery or the use of bone graft.
Reference: